Original Articles - Journal of Medicine and Medical Sciences ( 2019) Volume 10, Issue 2
Received: 20-Mar-2019 Published: 22-Apr-2019
Background: Thyroid nodules are seen in many patients today, and fine needle aspiration biopsy is required to identify these nodules. These biopsies are usually performed with ultrasound guidance. Because these procedures are painful in many patients, the need for anesthesia emerges in the Thyroid FNAB. Aim: In our study, we wanted to examine whether the use of ethyl chloride sprays, which are also known as coolant sprays, is an alternative to local anesthetic creams, which is a conventionally used method for these procedures.
Methods: This study included 77 patients who were admitted to the endocrinology outpatient clinic of Pamukkale University Medical Faculty (PAUTF) Hospital. In our study, we evaluated whether cold sprays containing ethyl chloride as an alternative method for local anesthesia to relieve pain in ultrasound-guided thyroid FNAB procedures in endocrinology outpatient clinic were useful for patients.
Results: When the patients were evaluated, patients divided into 3 groups as group made an operation with cooler spray as Group 1, patients implemented local anaesthetic cream tropically as Group 2 and patients who weren’t implemented any operation before and after the operation as Group 3. When Mc gill Melzack pain scale was compared, group 1 (n:32) took 54,19 group 2 (n:24) took 44 and group 3 (n:21) took 67,29 points.
In Group 2, it was found that the pain was the least felt and this value was statistically significant (p:0.0001). When VAS-NRS scores were examined, VAS values were found to be 4.46 in group 1 and 4.34 in group 2 and 4.33 in group 3 and there was no statistically significant result in this situation. But 10 minutes after the procedure in terms of VAS, the group 2 was lowest.
Conclusion: In conclusion, in our study, we found that ethyl chloride; cold sprays can be an effective alternative to local anesthetic creams as an alternative method of pain relief.
Local anesthesic, thyroid, fine needle aspiration
Thyroid nodules can be defined as lesions that appear radiologically different from the parenchyma around the thyroid gland (Ahmeti I, 2015). Thyroid nodules are one of the common problems in the community and palpabal nodules are present in 5% of the population and this rate can be increased to 70% by coincidentally detected nodules with ultrasound (Wong R, 2018).
These nodules, which are seen as high in the community should be excluded from malignancy for appropriate treatment management, although the likelihood of malignancy is relatively low.
The application of fine needle aspiration biopsy (FNAB) to diagnose common nodules is often preferred today (Liao L, 2018). FNAB can be performed in two different ways with palpation technique or ultrasound (USG) (Choong KC, 2018). FNAB may experience false negative results due to the experience of the clinician and the interpretation of the cytologist.
Although no method is recommended in the guidelines, USG's assistance is particularly valuable in nonpalpable nodules and cystic nodules (Erık KA, 2002). The result of FNAB can determine the likelihood of malignancy and cytological features have prognostic value in thyroid papillary carcinoma (Mustafa C, 2006).
The American guidelines recommend the use of USG as it facilitates finding the nodule, but with USG, FNAB increases the likelihood of some complications such as pain, anxiety and bleeding, infection, recurrent laryngeal nerve injury, and possible needle trauma (Stergios AP, 2009). Most patients usually tolerate pain and anxiety during the procedure (Lo WC, 2014). Therefore, the application of local anesthesia during FNAB is generally not recommended (Gharib H, 2006).
However, in some studies, local anesthetics (LA) were administered before FNAB in the presence of USG and the patient gave positive results in tolerating the procedure compared to the patient group who was not administered anesthetic (Kim DW, 2009). Since, there are many different clinical applications, the necessity of local anesthesia remains unclear (Choong KC, 2018). No study recommends the necessity of LA (Kim DW, 2009).
Cold spray application is not an application in thyroid fine needle aspiration biopsies. Sprays containing ethyl chloride, which is mostly used in dermatological and cosmetic fields, can be used for curette biopsies (Flynn A, 2016). Although there are not many studies in the literature on ethyl chloride, in the United States, hand surgeons used ethyl chloride in a very large group of patients (2083 patients) but they did not see any benefit before injection (Franko OI, 2016).
In a study conducted in Ireland, the use of ethyl chloride in dermatology clinic was evaluated and a snowball effect of 30 seconds before the procedure was stated. This short-term effect was well tolerated and procedures were successfully performed in dermatological interventions (Flynn A, 2016). In our study, we evaluated whether cold sprays containing ethyl chloride as an alternative method for local anesthesia to relieve pain in ultrasound-guided thyroid FNAB procedures in endocrinology outpatient clinic were useful for patients.
This study included 77 patients who were admitted to the endocrinology outpatient clinic of Pamukkale University Medical Faculty (PAUTF) Hospital. Perceptions of pain in the Mcgill-melzack pain scale were used for the perception of pain. Procedures to be applied to random patients before ultrasound-guided thyroid fine needle aspiration biopsy. In this study, the patients were contacted by phone and the approvals were given. The data was evaluated retrospectively.
These patients were divided into 3 different groups. Group 1 treated with local anesthetic cream, group 2 applied cooler spray and group 3 was placebo (no chemical substance applied) group.
Patients were divided into 3 groups by obtaining permission from the patients while Group 1 patients take into the operation after spraying cold spray to the neck area, Group 2 patients were taken into biopsy after implanting local anesthetic cream 10 minutes before the operation (EMLA cream %5=lidocaine Hcl +prilocaine).
The 3rd group was treated with no chemical agent. After this procedure, fine needle aspiration biopsy was applied to thyroid nodules in the presence of USG. After the procedure, patients were asked to evaluate the pain immediately before the procedure and this was done by VAS and visual pain scores (VAS) were asked to the patients 12 hours after the procedure. At the same time 10 minutes after the procedure, patients were asked to evaluate the pain conditions during the procedure.
For this, 3 groups were asked to describe the type of pain they felt during the procedure, how the pain was passed and the pain during the procedure with the McGill Melzack pain scale. The pain assessment (NRS) score was made by evaluating the patients from 1 to 10 after the biopsy, during the procedure and 12 hours after the procedure. Afterwards, the findings of the patients in 3 groups were collected and evaluated.
Mc Gıll Melzack Paın score
The McGill Melzack pain score is used to evaluate multidimensional pain. For pain assessment index, pain is a survey derived from the door control theorem (Donaldson GW, 1995). This questionnaire questions sensory and evaluative components of pain.
Visual analogue scale
Visual analogue scale (VAS) has been used to measure the quality of life and anxiety of intolerable amounts of pain since the 1920s. The patient's worst imaginable pain and no pain definitions are limited to a line with a length of 100 mm and are marked according to the patient's perception of the degree of pain (Hellera GZ, 2016). Value is given according to the distance. VAS is available in ratings with alternative numbers (Numeral Rating Scale (NRS)). VAS may be difficult to assess in very elderly patients, but it is a practical method for assessing pain in many patients today (Jensen MP, 1986).
Statistical analysis
In order to determine the number of patients to be included in the pre-study groups, the sample size was calculated. When 70 patients were taken for this study, 95% confidence was obtained with 95% power (Graphpad StatMate 2 Windows Program).
A total of 77 (± 10%) patients were planned to be included in the study group considering the possibility of possible loss in the process due to technical reasons. In this study, the data were analysed by SPSS 22 for Windows Corporation package program. Continuous variables are given as mean ± standard deviation (minimum value-maximum value) and categorical variables are given as number and percentage. Since parametric test assumptions were obtained, ANOVA test was used. Comparative T test was applied to the source of the meaningfulness within the group.
A total of 77 patients underwent thyroid FNAB in the polyclinic of PAUTF. When the demographic characteristics of these patients were evaluated, 71 patients were female and 6 were male. (92.2% F %7.8% M) The mean age of the patients was 47.58 years. The mean body mass index (BMI) of the patients was 28.34. Cognition pain detection criteria were determined according to the likert scale (Table 1).
| Demographic | Average ± s.s |
|---|---|
| Gender (F/M) (n (%)) | 71 (92.2%)/6 (7.8%) |
| Age | 47.58 ± 13.39 |
| VKİ | 28.34 ± 5.88 |
| Cognition* | 2.84 ± 1.06 |
Table 1. Demographic data.
When the patients were evaluated, patients divided into 3 groups as group made an operation with cooler spray as group 1, patients implemented local anaesthetic cream tropically as group 2 and patients who weren’t implemented any operation before and after the operation as group 3.
When Mc gill Melzack pain scale was compared, group 1 (n:32) took 54,19 group 2 (n:24) took 44 and group 3 (n:21) took 67,29 points. In Group 2, it was found that the pain was the least felt and this value was statistically significant. (p:0.0001).
When VAS-NRS scores were examined, VAS values were found to be 4.46 in group 1 and 4.34 in group 2 and 4.33 in group 3 and there was no statistically significant result in this situation.
When these groups were evaluated 10 minutes after the procedure in terms of VAS, the group 2 was lowest with VAS 1.76. (group 1:2, 03 ve group 3:3, 14) (p: 0.001) this was statistically significant in the perception of the decrease in the LA group of pain. 12 hours after the procedure, when the patients were asked to reach the phone with a score of pain, the VAS value of group 2 was 1.38 and the pain was the least. (Group 1:2, 06 group 3:3, 19) (Table 2).
| Group I (n=32) | Group II (n=24) | Control (n=21) | p | |
|---|---|---|---|---|
| Mcgill- melzack Pain Scale | 54.19 ± 7.87 | 44.00 ± 6.29 | 67.29 ± 10.89 | 0.0001* (Group I-control, Group II control) |
| VAS beginning | 4.46 ± 1.49 | 4.34 ± 1.27 | 4.33 ± 1.28 | 0.284 |
| VAS Post Treatment | 2.03 ± 1.52 | 1.76 ± 0.70 | 3.14 ± 1.46 | 0.001* (Grup I-kontrol, Grup II- Kontrol) |
| VAS after 12 hrs | 2.06 ± 1.11 | 1.38 ± 0.74 | 3.19 ± 1.40 | 0.0001* (Grup I-kontrol, Grup II- Kontrol) |
Table 2. Intergroup evaluation of pain scales.
When the focal point of the pain was evaluated in group 1, 11 patients felt deep pain, 11 patients stated pains as superficial and 10 patients stated their pains as both deep and superficial while in group 2, 7 patients felt deep pain, 9 patients felt superficial pain and 8 patients felt pain both deep and superficial.
In group 3, 7 patients felt deep pain, 6 patients felt superficial pain and 6 patients felt both deep and superficial pain. There hasn’t been any statistical meaning (Table 3 and Figure 1). While assessing how patients reduce pain, pain reduction methods are examined; as seen in the graph, cold application with rest and movement limitation was good for the pain of the patients but there was no statistically significant difference between them (Figure 2).
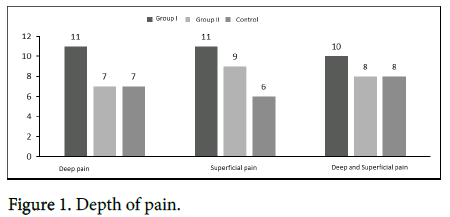
Figure 1: Depth of pain.
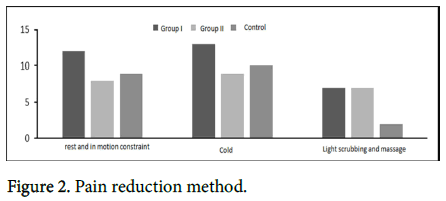
Figure 2: Pain reduction method.
| Focal point of the pain | Group I (n=32) | Group II (n=24) | Control (n=21) |
|---|---|---|---|
| Deep pain (n=25) | 11 | 7 | 7 |
| Superficial pain (n=26) | 11 | 9 | 6 |
| Deep and superficial pain (n=26) | 8 | 8 | 8 |
Table 3. Focal point of the pain.
In our study, pain scores were evaluated in 3 different groups and it was determined that there was a statistically significant pain reduction with local anesthetic group and in the pain group implemented cold spray and undoable implementation.
While VAS score was 4.34 before the procedure in the local anesthesia group, this score was found to be 1.76 after the procedure and this was statistically significant. At 12 hours after the procedure, VAS was the lowest in the local anesthetic group with 1.38. This difference was interpreted as local pain relief of thyroid fine needle biopsies (Figure 2). When combined with deep and superficial pain and pain scales were evaluated together (McKill), the lowest score of superficial pain in the melzack pain scale (49,92) was found to be statistically significant. The VAS criteria evaluated 10 minutes after the procedure were again, values in superficial pain and the others were statistically significant (Table 4). With these evaluations, we can see that the pain scales help us with the degree of pain before and after the procedure.
| Deep pain (n=25) | Superficial pain (n=26) | Deep and Superficial pain (n=26) | P | |
|---|---|---|---|---|
| Mcgill- melzack Pain scale | 56.04 ± 10.94 | 49.92 ± 12.33 | 63.81 ± 8.54 | 0.0001* (Group II- Control) |
| VAS introduction | 4.45 ± 1.25 | 3.92 ± 1.22 | 4.27 ± 1.64 | 0.318 |
| After VAS treatment | 2.52 ± 1.22 | 2.02 ± 0.70 | 2.87 ± 1.65 | 0.001* (Group II- Control) |
Table 4. Comparison of scales with depth of pain.
Thyroid nodules are a common clinical problem and palpable patients are observed in 5% of the population. Detection by USG is 70%, especially in elderly patients (Wong R, 2018). The importance of thyroid nodules is important in evaluating the functions of the thyroid gland, in diagnosing local neck symptoms and in detecting malignancies (Wong R, 2018). Fine needle aspiration biopsy (FNAB) is an effective, reliable and mandatory procedure for the evaluation of these thyroid nodules (Gursoy A, 2007). This is a short-term procedure and is a very sensitive cytological indicator. It is accepted as the gold standard method for diagnosis that can be applied to walking case (Demirci H, 2010). Administration of these procedures with USG is preferred in non-palpable thyroid nodules. Ultrasound is inevitable in detecting malignancy with clinical ability and physician experience (Kim DW, 2009). Although it requires more experience than palpation, USG-guided thyroid FNAB is more preferred today as it reduces insufficient material and false negative results (Mustafa C, 2006). In a study evaluating 215 patients, biopsies performed with USG and biopsies with palpation method were taken while biopsies of thyroid nodules were taken. Each nodule was evaluated with both palpation and USG, and consequently the rate of inadequate material intake was found to be statistically significant in the palpation method. Again, the same study evaluated the cost status between the two methods and the FNABs performed with USG were less expensive than the other group (Mustafa C, 2006). Again, carcinoma of 106 patients and hurtle cell metaplasia of 3 patients were detected with the help of USG (Ahmeti I, 2015). Many studies show us that thyroid nodules are a practical method for the diagnosis of malignancy and biopsy diagnosis. It reminds us that USG is the gold standard method in biopsy when applied by experienced physicians (Erık KA, 2002).
In a US study, 1128 patients were diagnosed with malignancy in biopsies performed for 6 years, and how valuable the USG was in the diagnosis of undiagnosed thyroid nodules (Erık KA, 2002). Biopsy is performed routinely without anesthesia. Although it is known that the patient is not painful during the procedure, it is believed that the patients have less sensitivity when local anesthesia is applied (Demirci H, 2010). Because biopsy can become anxiety and phobia especially in patients with fear of needles (Gursoy A, 2007). Although pain control is performed with many different methods, local anesthesia is frequently applied by cutaneous methods (Gursoy A, 2007; Demirci H, 2010). Some studies have even applied sedation method in thyroid biopsies (Kholmatov RM, 2018). In the literature, many studies have been done on the use of local anesthetics in thyroid biopsies and the opinions about its usefulness are controversial. In a study evaluating 99 patients, 50 patients with USGguided thyroid FNAB were treated with local anesthetic cream and the patients were evaluated by VAS scoring after the procedure. When NRS and VRS were compared in the placebo group, it was found that the group implemented local anesthesy had less pain in 3 different pain scoring groups (Gursoy A, 2007). In another study evaluating the usefulness of local anesthetics in biopsies with USG guided biopsies; local anesthesia was performed in 50 patients where the size of the nodules was almost the same. In 50 patients, no anesthetic agent was administered. There was more pain in one entry in the patient group who applied local anesthetic in 3 different pain score evaluations (VRS, NRS and VAS) in the biopsies by experienced physicians. These authors have argued that local anesthesia is not necessary for thyroid FNAB (Kim DW, 2009). A recent study involving a large population of patients compared local anesthesia with sedation in thyroid FNAB and 66 of 860 patients underwent sedation during the procedure. In this study performed in USA, performance was evaluated during the procedure but no pain score was used. No significant difference was found between the two groups in terms of complications and biopsy, and although the patients who were treated with sedation were more satisfied, there was no statistically significant difference in sedation complication or easing the procedure (Kholmatov RM, 2018). In 2 different studies performed in our country, it is observed that local anesthetic applications applied before the FNAB provide a significant reduction in pain scores (Gursoy A, 2007). In his study Gursoy et al., the rate of painlessness was 90.9% in the LA group and this rate was 44.2% in the placebo group and the benefit of local anesthesia in the comfort of patients was mentioned (Gursoy A, 2007). However, in a study conducted in the same region, no significant difference was found between the local anesthetic cream-treated pain scores and the placebo group in 25 of 50 female patients (Demirci H, 2010). In our study at 12 hours after the procedure, VAS was the lowest in the local anesthetic group with 1.38. This difference was interpreted as local pain relief of thyroid fine needle biopsies.
Many different clinical experiences and applications still suggest the necessity of local anesthesia in biopsies. Pain scoring systems can provide us with more objective results in evaluating these applications. In a study evaluating pain levels for biopsy applications in neck masses, the visual analog scale (VAS), Numeric Rating Scale (NRS) and verbal rating scale (VRS) were compared in 3 different neck biopsies. (thyroid nodules, lymph nodes and salivary gland lesions). Pain scores were evaluated during the procedure and after 5 minutes. It was found that lymph node biopsy was more painful by patients. However, there were no discrepancy or differences regarding the difference of pain scores (Lo WC, 2014). As in the present study, it was shown that thyroid nodules may be painful, but only 11% of patients prefer this anesthetic method when asked if they want local anesthesia and it is stated that 89% of patient doesn't need for anesthetic method in thyroid FNAP (8Again in a study in which 183 patients evaluated pain scores for biopsies, it was reported that LA administration reduced moderate pain and facilitated the procedure (Liao L, 2018). In our study, we focused on how pain affects patients with two different scale VAS and Mc gill Melzack pain scores used for the evaluation of pain. As with all studies, while VAS was asked to draw points between 1 and 10 points, the depth of pain and sensory, affective and evaluative aspects of pain were determined by Mc Gill melzack scoring system. This scale has not been applied to the thyroid FNAB in the literature, and we believe that this scale can help to differentiate the pain and to determine the pain reduction methods on a patient basis.
The use of ethyl chloride in pain reduction in the literature is quite common. Ethyl chloride applied for more dermatological and cosmetic treatments is known as short-term analgesic method with spraycooling effect (Flynn A, 2016). In orthopedic attempts, the use of ethyl chloride is common. In a study of 60 patients who underwent upper extremity electromyography, ethylchloride and placebo sprays were applied to reduce pain before the procedure and patients were found to have lower VAS scores in patients treated with ethyl chloride than those with VAS. In addition, it was found that this application of ethyl chloride did not cause any reduction in response during the procedure (Moon YE, 2014). Again, the hand surgery study has evaluated the use of ethyl chloride in orthopedic intramuscular injections, but it has been found that there is no benefit in reducing the injection pain of ethyl chloride (Franko OI, 2016). Occasionally, the use of ethyl chloride instead of lidocaine creams has also been introduced in botox applications. In a study of 45 female patients in the botox application EMLA cream was compared with ethyl chloride spray. In Group 1 of the patients divided into 3 groups treated only with lidocaine, 2. Group treated with ethyl chloride spray Group 3 treated with lidocaine cream on one half of the face and ethyl chloride spray on the other half. Pain sensitivities were evaluated with VAS. Among the groups, the group with the least pain felt was Group 1. The benefit of ethyl chloride before botox application was determined in this study (Irkoren S, 2015). In some studies, the use of ethyl chloride in gynecological processes was compared with lidocaine. In a study evaluating 120 patients who underwent catheter insertion, intradermal lidocaine group had less pain compared to ethyl chloride spray group and VAS values were lower in patients with lidocaine (Armstrong P, 1990).
In our study, we compared the use of ethyl chloride with the lidocaine topical cream for thyroid FNAB which has not been previously applied in the literature. In our study, in the group we applied ethyl chloride spray as the first group, VAS value was 2.06 after 10 minutes and this value was 1.76 in the topical local anesthetic group. In our evaluations, although ethyl chloride spray is less effective than local anesthetic creams, In this study we found that VAS values in the placebo group (group 3 VAS 3.19) were higher than the two groups, and that ethyl chloride sprays, also known as refrigerant spray, could be an alternative for thyroid FNABS. These investigations and findings suggest the benefits of local anesthetics in the thyroid FNAB accompanied by USG and suggest that ethyl chloride spray may be an alternative to relieve patient's pain. We think that more comprehensive studies are needed.
Ethical approval statement: This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent statement: Does not apply.
Financially supporting: No financial support was received from any institution for this study.
Data availability statement: The data used to support the findings of this study are included within the article.
Conflict of interest: All authors have worked together for this article and there is no conflict of interest.